According to “The New York Times” Ebola virus could reach 1,4 million infections, by January 2015, in four months. Impressive. How do they get this figure? By “leveraging” on some “projections” from CDC (USA health related organization) who, in turns, “tailor” some epidemiological figures coming from the WHO (World Health Organization, part of the UN establishment).
The CDC provided, thanks to a powerful computer simulation (likely without any human intelligence contribution), two figures: a best and a worst-case scenario. In the worst case scenario the outbreak of Ebola could reach 1,4 million people; in the best case scenario the outbreak could reach 21,000 people. A worst-case scenario that is 65 times worse than the best scenario? Reasonable, isn’t it?
Some facts. What is Ebola? It is a virus, than can infect a sane human body by direct contact with infected fluids or materials; and it can lead to death. Fine so far.
How much this is this virus epidemic and how deadly is it? According to WHO: “Infection occurs from direct contact through broken skin or mucous membranes with the blood, or other bodily fluids or secretions (stool, urine, saliva, semen) of infected people. Infection can also occur if broken skin or mucous membranes of a healthy person come into contact with environments that have become contaminated with an Ebola patient’s infectious fluids such as soiled clothing, bed linen, or used needles.“
This implies that Ebola has a low contagion potential, because can be physically contained. It is not transmitted via air (proximity with infected human) or via external agent (as mosquitos in the case of malaria). According to the WHO, the Ebola outbreaks records (from 1976 up to 2012) cumulate in 36 years 2387 cases in total, 1590 of which resulted in deaths, with a death ratio of 67%.
Mass media in these days used to claim a deadly potential ranging between 50% and 95%. How do they raise the deadly figure? Pretty simple. Let’s imagine in country “X” we have, from January to March, 1 reported case of Ebola and the patient dies; in this case the mortality rate is 100%. And let’s assume that from March to December we have 99 cases of Ebola with 65 deaths; in this case we have 66% death rate. The trick is almost done, because we can draw the conclusion that “the death ratio ranges between 66% and 100%”, got it? While actually the mortality rate is 66/100, in other words 66%. That’s the power of math.
Those data, come from the countries with higher risk: Congo, Sudan, Uganda, Gabon, Cost d’Ivoire.
The fact that in the 5 above countries the reported Ebola human infections amounts to less than 3000 in 36 years, does not mean that the actual infections are that low. Many cases could have not been reported. However, it is important to note that in 36 years the total number of infected people ranges from a minimum of 0 cases up to a maximum of 425 cases (year 2000, Uganda) without showing evidence of an increasing trend. Emblematic is the case of Congo, where the Ebola reported infections ranging from a maximum level of 318 cases in 1976 down to 57 cases in 2012 (68 cases in 2014).
Then, what these data should teach us? A few things:
- even if we assume that the actual infection level is higher than what is reported, the real one cannot be higher than the measured by several orders of magnitude, because otherwise the infection would have already exploded in 36 years of incubation
- there is no increasing trend, at all, and apparently figures contraddict the idea of a deadly and contagious virus out of control. Actually, this is not surprising and instead it is consistent with the way the virus works.
- In all countries monitored, the number of reported cases decreases steadily from the initial detected outbreak figures; this is consistent both with the not so high infection potential of the virus and with the fact that traditional procedures of containment are somewhat effective in reducing the infection and thus the death toll:
- In Congo were registered 318 cases in 1976 with mortality rate of 88%, become 57 cases in 2012 with mortality rate of 51%
- In Sudan were registered 284 cases in 1976 with mortality rate of 53%, become 17 cases in 2004 with mortality rate of 41%
- In Uganda were registered 425 cases in 2000 with mortality rate of 53%, become 31 cases in 2004 with mortality rate of 67%
At this point you will have noticed one thing for sure. In the above monitored countries, do not appear neither Liberia nor Sierra Leone, the countries that today make the first page of Ebola bulletin. Indeed only in 2014, apparently, Ebola outbreaks manifested in Nigeria, Guinea, Liberia, and Sierra Leone. According to the WHO report, these countries in 2014 accounted for 3486 confirmed cases and 1496 deaths, with an average death ratio of 43%. The country with the highest infection level is Sierra Leone (1745 cases), the one with highest death ratio is Guinea (56%).
 Then WHO takes in account the “probable” cases of Ebola infections, meaning cases with symptoms compatible with Ebola and have linking with other Ebola cases. With the “probable cases” the count of “cases” grows up to 5135 and the deaths raises up to 2152 (42% death rate). This leads to the following histogram.
Then WHO takes in account the “probable” cases of Ebola infections, meaning cases with symptoms compatible with Ebola and have linking with other Ebola cases. With the “probable cases” the count of “cases” grows up to 5135 and the deaths raises up to 2152 (42% death rate). This leads to the following histogram.
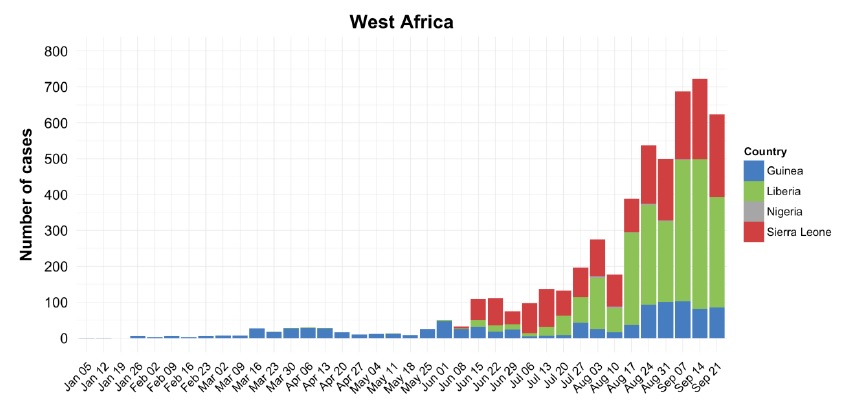
As you can see above, the count has ramped up quickly in the last months, and before 2014 was not existent. How is it possible? It is reasonable to assume that, given the proximity of the countries implied, the virus existed already in Liberia, Guinea and Sierra Leone, and with that also humans infected.
At first glance the graph suggests an exponential growth, typical of epidemic phenomena out of control. However, how that can it be possible given the limited time span (4 months) and the low contagious level of the virus, as demonstrated by the other countries where such exponential growth did not happen, not in just 4 months but in 36 years?
Indeed, it is not possible.
And if you look more carefully at the graph, you’ll notice that in the last weeks the trend seems to have stabilized. Is it because the infection spread stopped? We do not know. Likely the infection proceeds more or less at steady rate, a slow growth rate, as the 36 years known history of the virus teaches.
The real point is that the period of observation is too short, and what the numbers really “measure”, is the development of the observation system and not the development of the epidemologic system to be observed.
Indeed, this is the reason why WHO’s director Christopher Dye states “We’re beginning to see some signs in the response that gives us hope this increase in cases won’t happen”, acknowledging that the predictions come with a lot of uncertainties; “this is a bit like weather forecasting. We can do it a few days in advance, but looking a few weeks or months ahead is very difficult.”
Then, how did CDC come to the 20,000+ infections best case scenario figure? Well, that figure actually can be reasonable considering the actual numbers (around 5,000) and taking in consideration that a significant amount of infection cannot yet be in the record. But how can they assume as credible the 1,4 million figure, knowing the 36 years old history of previous outbreaks in other countries?
It cannot be a mistake made by specialists of epidemiology.
Ebola is not a global emergency, period. Comparatively speaking, Malaria affects between 200 and 300 million people worldwide, and roughly 700 thousands die every year. Malaria has a lower mortality rate compared to Ebola but is much more pervasive, and it is endemic. Notably, Sierra Leone, counting less than 1800 Ebola cases and less than 600 Ebola deaths, accounts for almost 8000 people dying every year of Malaria; in Guinea the Malaria toll accounts for 9000 deaths/year, in Liberia for over 2000 deaths/year and in Nigeria for over 120,000 deaths/year.
How did it happened that a virus, Ebola, known since 1976 with available containment and prevention methodologies and cures, has become an emergency, despite the low death toll (in absolute terms and comparative terms) and the low infection potential?
Moreover, given the above, why there is a push for vaccines? Vaccination procedures are meant to address high-risk diseases (and admittedly this is the case) with high infection potential (this is not the case). There is no evidence of an emergency, so why to rush?
Cui prodest?
Given the above facts, now it is time for my speculations. Has the “Ebola” outbreak been manufactured? No, but in a sense, yes!
To assume that Ebola has been engineered in laboratories, and thus released for achieving obscure objectives, is speculation without evidences.
Nevertheless, yes, it has been manufactured, manufactured by the mass media.
Biotech industry is one of the major bet of western economy, especially US ones; such enterprises do not create the disease and then the cure; they work the other way around. They discover a “treatment” and then they “market” the relevant disease. A relevant case is AHDH, and US citizens should know.
Ebola seems to fit nicely this scenario; however, the push from Obama for a vaccine, the marketing of the US as the ones that will save Africa people from their bad fate, suggest that multiple more strategic “interests” are looking for their way…
For sure, the biotech companies have to pay back their shareholders. However, there is more. Africa is the new greenfield, for the US and for China, two countries who are competing in the conquest of the natural resources of the only continent without a real sovereignty. China is gaining traction, US have very little to offer now, and probably health is the only card left that can be meaningful in Africa.
Obama administration has just recently established strategic business agreements in Liberia, and in October Liberia will host the local national elections. This is not a coincidence. The vaccines coming from the old American friend are a good tool to consolidate a long lasting partnership between US and Liberia, while at the same time to support the political campaign of the African “friends”. Obviously, in case things should go wrong, well, the military camps are already there, just in case…
I believe this is the African Blueprint.
